General Neurosurgery
Case Report
- Department of Neurosurgery, Burns and Trauma Center, Ben Arous, Tunis, Tunisia
Correspondence Address:
Aslam Hentati
Department of Neurosurgery, Burns and Trauma Center, Ben Arous, Tunis, Tunisia
Aslam Hentati
Department of Neurosurgery, Burns and Trauma Center, Ben Arous, Tunis, Tunisia
DOI:10.25259/SNI-234-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.Abstract
Background:The Type I malformations are supposed to be the result of mesodermal defects that create a congenitally small posterior fossa. However, Chiari malformation could be also “iatrogenic” and then called “acquired” Chiari I malformation. In this study, the authors report the clinical feature of a patient who developed a Chiari I malformation after lumboperitoneal shunt.
Case Description:A 35-year-old woman has been suffering from idiopathic intracranial hypertension and rhinorrhea due to an anterior skull base defect. A valveless lumboperitoneal shunt followed by surgical closure of the defect was performed. Six months later, she suffered from major continuous occipital headaches. The neurological examination found a mild cerebellar gait ataxia and cerebellar dysarthria. The cerebral magnetic resonance imaging (MRI) showed a ptosis of the cerebellar tonsils and a disappearance of the cisterna magna; there was no syringomyelia. This herniation was not present before shunt was performed. A replacement of the lumboperitoneal shunt with a pressure-regulated valve chamber was performed. After a 1-year follow-up, the patient reports a marked decrease of the headache as well as the ataxia, and the last cerebral MRI showed resolution of the Chiari I malformation.
Conclusions:Symptomatic acquired Chiari malformation with or without syringomyelia as a delayed complication after lumbar shunting is a rare complication, particularly reported in the pediatric population, but could also occur to adult patients. Treating these patients by correcting the shunt’s valve could be enough, but should be monitored, as it may fail to resolve the Chiari malformation even years after treatment.
Keywords: Chiari malformation, Complication, Lumbar shunt
INTRODUCTION
The Chiari I malformation was first described by Chiari, in 1891.[ 2 ] It is characterized by the presence of cerebellar tonsils in the upper cervical canal while the fourth ventricle remains above the foramen magnum.[ 2 ] The Type I malformations are supposed to be the result of mesodermal defects that create a congenitally small posterior fossa.[ 12 ] However, Chiari malformation could be also “iatrogenic” and then called “acquired” Chiari I malformation.[ 12 , 21 ] In fact, the term of acquired Chiari malformation (ACM) was used by Payner et al. in the presence of the herniation of cerebellar tonsils subsequent to the documentation of a normal hindbrain in prior brain imaging.[ 14 ] It was mainly described after cerebrospinal fluid (CSF) shunting, first after lumboperitoneal shunting, and lately recognized after supratentorial shunting.[1 , 3 , 5 , 14 ]
In this study, we report the clinical features of a patient who developed a Chiari I malformation after lumboperitoneal shunt.
CASE REPORT
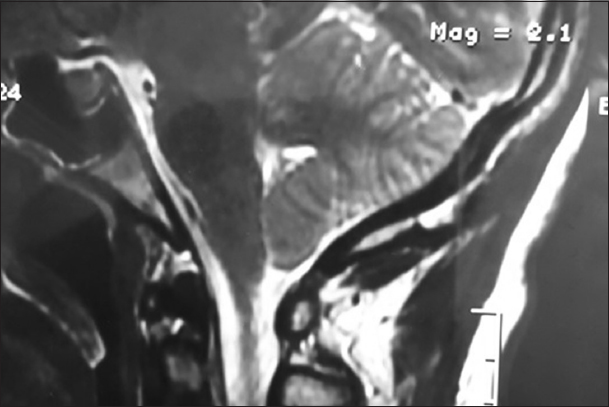
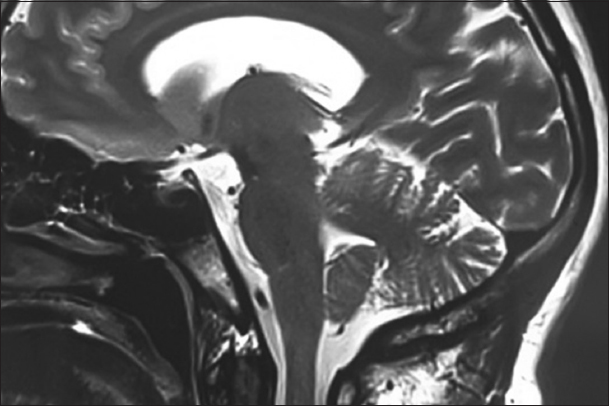
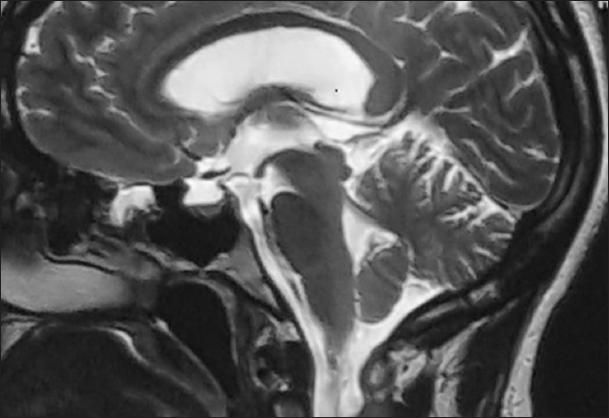
A 35-year-old woman has been suffering from idiopathic intracranial hypertension for 8 years. For 3 years, the patient has had rhinorrhea due to an anterior skull base defect. A valveless lumboperitoneal shunt followed by surgical closure of the defect was performed. Six months later, she suffered from major continuous occipital headaches with nauseas. The neurological examination found a mild cerebellar gait ataxia with limb incoordination and cerebellar dysarthria. Cranial nerve examination was normal. The cerebral magnetic resonance imaging (MRI) showed a ptosis of the cerebellar tonsils and a disappearance of the cisterna magna [ Figure 1 ]. This herniation was not present before shunt was performed [ Figure 2 ]. A replacement of the lumboperitoneal shunt with a pressure-regulated valve chamber was implemented. After a 1-year follow-up, the patient reports a marked decrease of the headache as well as the ataxia. The last cerebral MRI showed resolution of the Chiari I malformation [ Figure 3 ].
DISCUSSION
Chiari malformation type I (CM-I) has traditionally been defined as a dislocation of the cerebellar tonsils 5 mm or more below the foramen magnum on sagittal MRI.[ 11 ] CM-I is often associated with basilar invagination, as described by Liao et al., as they represent the most common craniovertebral junction malformations (CVJ).[ 10 ] Furthermore, they can be associated with other miscellaneous CVJ malformations such as platybasia or more rarely a defect of closure of the posterior arch of C1, an occipitalization of the atlas, a C1–C2 dislocation, and C1–C2 fusion.[ 4 , 10 ]
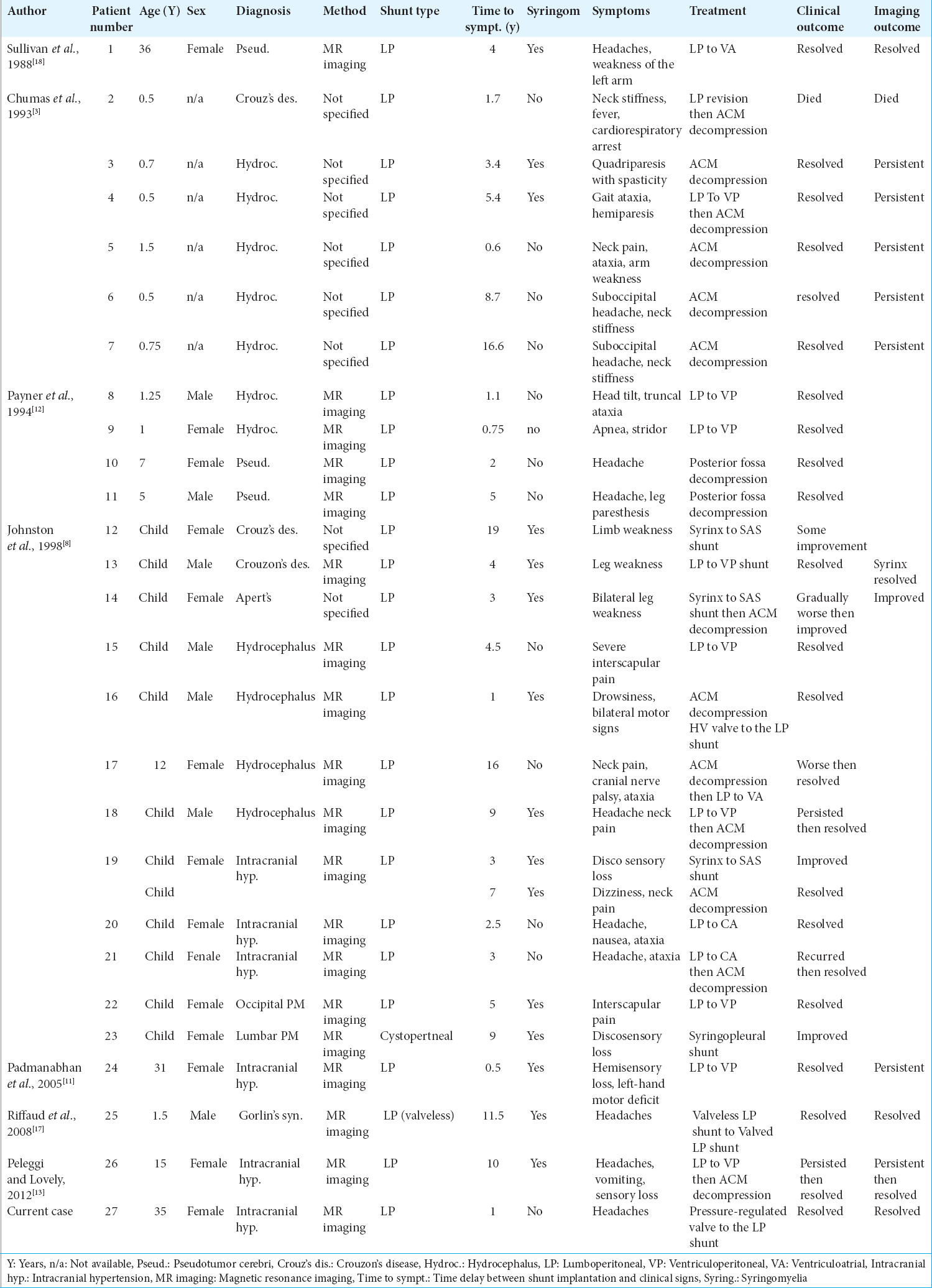
Unlike the “classic” CM-I, ACM is defined by the herniation of cerebellar tonsils subsequent normal hindbrain in prior brain imaging, and it is not related to CVJ malformations.[ 14 ] ACM was first described by Hoffman and Tucker, in 1976, as a late complication of lumboperitoneal shunt.[ 7 ] To the best of our knowledge, 36 patients of ACM due to lumboperitoneal (LP) shunts have been reported since 1976.[ 3 , 7 , 8 , 13 - 15 , 17 , 18 , 21 ] Among them, 27 cases are summarized in the table below. These patients were selected as they present enough information about their imaging (MRI and/or computed tomography scan), clinical data, and postoperative outcome.
The incidence of ACM due to LP shunt varies in different series. Chumas et al. reviewed a series of 143 patients to determine the incidence of ACM and found that the incidence of hindbrain herniation may be as high as 70% in asymptomatic patients with LP shunts.[ 3 ] Five of these patients became symptomatic and required Chiari decompression.[ 3 ] During their follow-up period, which is about 5.7 years, there was one shunt-related death due to unsuspected tonsillar herniation.[ 3 ] However, in two other series of 25 patients by Rekate and Wallace and of 74 patients by Wang, no patient developed an ACM.[ 16 ] In another series of 70 patients treated with LP shunting for pseudotumor cerebri, Johnston et al. reported an incidence of an ACM in 11 patients.[ 8 ] Eight of them were asymptomatic and three required treatment.[ 8 ] Despite the variability of these results, ACM due to LP shunting should be considered, even if it is mostly asymptomatic. However, it should require a long follow-up due to the possible late onset of the symptomatology.[ 3 , 8 ]
All reported patients with ACM were children, except for the case described in this paper and the one reported by Padmanabhan et al.[ 13 ] Most of the symptoms were a manifestation of chronic tonsillar herniation (21 patients; 80%) (i.e., occipital and posterior cervical pain, long-track deficits, lower cranial nerve palsies, brain stem dysfunction, and cerebellar syndrome), whereas symptoms related to syringomyelia were less frequent (i.e., sensory loss or weakness in upper limbs).
ACM with or without syringomyelia had been noted after lumbar shunting regardless of the underlying etiology[ 8 ] [ Table 1 ]. It was mostly described in cases of pseudotumor cerebri and communicating hydrocephalus.[ 3 , 7 , 8 , 13 - 15 , 17 , 18 ,21 ]
While the cause of the ACM is debatable, most authors consider that it is a result of CSF pressure differentials across the cranial cervical junction, created by the drainage.[ 8 , 12 , 15 ] According to Johnston et al., the pathogenesis of syrinx formation may be explained by the hydrodynamic theory, as the lumbar shunt can be responsible of the disorders of CSF circulation.[ 8 ] Johnston et al. also reported one patient (number 14 in the table) having syrinx formation before ACM suggesting that “Chiari malformation may follow rather precede syrinx formation” in some cases.[ 8 ]
The “classic” CM-I is being increasingly diagnosed, but its optimal surgical treatment remains controversial.[ 9 , 19 , 20 ] Transoral odontoidectomy followed by occipitocervical fixation is a used approach to relieve ventral compressions.[ 6 , 20 ] Congenital CM-I is most treated by surgical posterior fossa decompression.[ 7 , 19 ] The traditional technique was to perform a suboccipital craniotomy and creating an artificially enlarged cisterna magna, suturing dural edges to the divided suboccipital muscles with wide arachnoid dissection.[ 22 ] A modification of this technique includes dural plasty, or with dura splitting or bone-only decompression.[ 9 , 19 ] Suboccipital craniotomy and opening the dura without opening the arachnoid, as described by Lavorato et al., is trending to be a good surgical strategy that can lead to an improvement of syringomyelic cavities.[ 9 ]
As for ACM due to LP shunt, the number of reported cases (27) is too limited to make clear and undoubtful therapeutic recommendations, but three possible strategies have been described:
To put a valve to a valveless shunt.
To resite the shunt.
To decompress the craniocervical junction.
Putting a valve to an LP shunt or resiting it could be an efficient solution to isolated ACMs. However, these techniques could not be enough when ACM is associated with syringomyelia, as symptoms did not resolve or could even get worse after a short or long follow-up. Craniocervical junction’s decompression could be required days or even years after shunt revision. It is also reported that isolated ACM could be treated by posterior fossa decompression alone, with good clinical and radiological outcome. Thus, a good and long follow-up after surgery is required, as a clinical relapse could lead to recite the shunt. Sullivan et al. and Riffaud et al. (patients number 1 and 25) reported a good recovery of patients having an ACM associated with syringomyelia after putting a valve to an LP shunt or resisting it.[ 17 , 18 ] However, the follow-up was not long enough (6 and 18 months), as a relapse could happen years after initial treatment (patients number 17 and 19).[ 8 , 17 , 18 ] Putting a pressure-regulated valve for the case reported in this paper is believed to be efficient. It was an isolated ACM, and symptoms resolved with a reascension of cerebellar tonsils. However, longer follow-up could also be required like for the other reportedly treated ACMs.
CONCLUSIONS
Symptomatic ACM, a rare complication of lumbar shunt, is particularly described in the pediatric population but could also occur to adult patients. The review of these reported cases suggests that the association with syringomyelia could be decisive about the need of decompression of the craniocervical junction.
Patients treated by only correcting the lumbar shunt should be monitored, as a relapse of the complication could happen years after initial treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Caldarelli M, Novegno F, Di Rocco C. A late complication of CSF shunting:Acquired Chiari i malformation. Childs Nerv Syst. 2009. 25: 443-52
2. Chiari H. Ueber veränderungen des kleinhirns infolge von hydrocephalie des grosshirns. Dtsch Med Wochenschr. 1891. 42: 1172-5
3. Chumas PD, Armstrong DC, Drake JM, Kulkarni AV, Hoffman HJ, Humphreys RP. Tonsillar herniation:The rule rather than the exception after lumboperitoneal shunting in the pediatric population. J Neurosurg. 1993. 78: 568-73
4. Ciappetta P, Signorelli F, Visocchi M. The role of arachnoid veils in chiari malformation associated with syringomyelia. Acta Neurochir Suppl. 2019. 125: 97-9
5. Di Rocco C, Velardi F. Acquired chiari Type l malformation managed by supratentorial cranial enlargement. Childs Nerv Syst. 2003. 19: 800-7
6. Dickman CA, Locantro J, Fessler RG. The influence of transoral odontoid resection on stability of the craniovertebral junction. J Neurosurg. 1992. 77: 525-30
7. Hoffman HJ, Tucker WS. Cephalocranial disproportion. A complication of the treatment of hydrocephalus in children. Childs Brain. 1976. 2: 167-76
8. Johnston I, Jacobson E, Besser M. The acquired chiari malformation and syringomyelia following spinal CSF drainage:A study of incidence and management. Acta Neurochir (Wien). 1998. 140: 417-27
9. Lavorato L, Spallone A, Visocchi M. Surgical treatment of chiari malformation in adults:Comparison of surgical techniques described in the literature and our experience. Acta Neurochir Suppl. 2019. 125: 139-43
10. Liao C, Visocchi M, Zhang W, Li S, Yang M, Zhong W. The relationship between basilar invagination and chiari malformation Type I:A narrative review. Acta Neurochir Suppl. 2019. 125: 111-8
11. Milhorat TH, Chou MW, Trinidad EM, Kula RW, Mandell M, Wolpert C. Chiari i malformation redefined:Clinical and radiographic findings for 364 symptomatic patients. Neurosurgery. 1999. 44: 1005-17
12. Nishikawa M, Sakamoto H, Hakuba A, Nakanishi N, Inoue Y. Pathogenesis of chiari malformation:A morphometric study of the posterior cranial fossa. J Neurosurg. 1997. 86: 40-7
13. Padmanabhan R, Crompton D, Burn D, Birchall D. Acquired chiari 1 malformation and syringomyelia following lumboperitoneal shunting for pseudotumour cerebri. J Neurol Neurosurg Psychiatry. 2005. 76: 298-
14. Payner TD, Prenger E, Berger TS, Crone KR. On the pathogenesis of syringomyelia:A review. J R Soc Med. 1994. 73: 798-806
15. Peleggi AF, Lovely TJ. Treatment of delayed chiari malformation and syringomyelia after lumboperitoneal shunt placement:Case report and treatment recommendations. Surg Neurol Int. 2012. 3: 101-
16. Rekate HL, Wallace D. Lumboperitoneal shunts in children. Pediatr Neurosurg. 2003. 38: 41-6
17. Riffaud L, Moughty C, Henaux PL, Haegelen C, Morandi X. Acquired chiari i malformation and syringomyelia after valveless lumboperitoneal shunt in infancy. Pediatr Neurosurg. 2008. 44: 229-33
18. Sullivan LP, Stears JC, Ringel SP. Resolution of syringomyelia and chiari i malformation by ventriculoatrial shunting in a patient with pseudotumor cerebri and a lumboperitoneal shunt. Neurosurgery. 1988. 22: 744-7
19. Villa A, Imperato A, Maugeri R, Visocchi M, Iacopino DG, Francaviglia N. Surgical treatment in symptomatic chiari malformation Type I:A series of 25 adult patients treated with cerebellar tonsil shrinkage. Acta Neurochir Suppl. 2019. 125: 125-31
20. Visocchi M, Trevisi G, Iacopino DG, Tamburrini G, Caldarelli M, Barbagallo GM. Odontoid process and clival regeneration with chiari malformation worsening after transoral decompression:An unexpected and previously unreported cause of “accordion phenomenon.”. Eur Spine J. 2015. 24: 564-8
21. Welch K, Shillito J, Strand R, Fischer EG, Winston KR. Chiari i “malformations” an acquired disorder?. J Neurosurg. 1981. 55: 604-9
22. Williams B. Surgery for hindbrain related syringomyelia. Adv Tech Stand Neurosurg. 1993. 20: 107-64
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου