blunt rupture of the heart, prompted this review. History. The first ... cardiac rupture, in a male victim of a motor vehicle accident who sustained a tear of the right atrial-superior vena caval ... chamber: right atrium, 36; left atrium, 30; right ventricle,.
Jun 19, 2018 - A severe complication from blunt cardiac trauma is cardiac chamber ... motor vehicle collisions (MVC), pedestrians struck by motor vehicles and ...
A fifty-year-old man presents after high speed motor vehicle crash. On arrival, he ... Blunt cardiac rupture is not evenly distributed between chambers. In a 5-year ...
Blunt cardiac injury is involved in up to 20% of all motor vehicle collision deaths. ... blood flow to the heart from the inferior vena cava with chamber rupture due ...
Blunt Cardiac Injury
Type Size
Introduction
Blunt cardiac injury (BCI) refers to injury sustained due to blunt trauma to the heart. The manifestations of such range from clinically silent, transient arrhythmias to deadly cardiac wall rupture. The absence of a clear definition and gold standard for laboratory testing make the diagnosis of blunt cardiac injury difficult. Treatment is tailored to the severity of injury and ranges from EKG monitoring to sternotomy with complex surgical repair.
The true incidence of BCI is unknown as reported rates vary greatly in the literature, ranging anywhere between 8 and 71%. Blunt cardiac injury is involved in up to 20% of all motor vehicle collision deaths. Although it occurs in only 20% of all blunt thoracic trauma patients, in patients with severe thoracic injury or multiple injuries, the incidence of BCI may be as high as 76%. Clinical studies looking at BCI in chest and abdominal trauma report incidences significantly lower than in autopsy series. This may suggest either that subtler forms of cardiac injury are underdetected when symptoms are minimal, or that many patients with significant BCI die in the field from cardiac or associated traumatic injury. In 2004 Schultz et al found myocardial contusion to be the most commonly reported blunt cardiac injury (60-100%). The distribution of injury amongst the different heart chambers relates to the anterior positioning of the right sided chambers in the chest. RV injury and RA injury are more common (17-32% and 8-65%, respectively), whereas left sided lesions are less frequent (LV~ 8-15%, LA 0-31%). Septal, coronary artery, and valve injuries occur even more rarely, with only a few case reports documented in the literature.
Mechanism of Injury
Because the heart is well encompassed within the bony thorax comprised of ribs and sternum, it requires significant force to cause BCI. This is seen most frequently in motor vehicle crashes and cases of pedestrians struck by motor vehicles. Other mechanisms, such as falls, crush injuries, assault, and sports related injuries with direct blows to the chest also contribute. Alternatively, severe abdominal compression can lead to rapid increase in blood flow to the heart from the inferior vena cava with chamber rupture due to a sudden increase in intracardiac pressure.
Blunt coronary artery injuries are exceedingly rare but may occur with direct impact leading to intimal disruption and thrombosis. This occurs almost always in conjunction with severe myocardial contusion, usually involving the left anterior descending artery as it lies anterior in the chest beneath the sternum. Sequelae from such injuries may be devastating, and can include myocardial infarction, production of emboli, arrhythmia, ventricular failure, and delayed ventricular rupture.
Valve injuries are equally infrequent and are due to compressive forces of blood during contraction that leads to valve, chordae tendinae, and papillary muscle rupture. The aortic valve is most commonly involved, followed by the mitral. Such injuries usually manifest as a combination of left ventricular dysfunction and cardiogenic shock.
Blunt pericardial rupture is rare but may be the most severe form of blunt cardiac injury. It results from both direct impact to the chest was as well as pressure alterations from compressive force to the abdomen, leading to laceration of the pericardium on both the diaphragmatic and pleural surfaces. This usually occurs parallel to the phrenic nerve and can lead to herniation of the heart into the thoracic or abdominal cavity and well as of torsing of great vessels, with subsequent cardiac arrest and death.
BCI is often part of multi system trauma and is most commonly associated with other thoracic injuries, such as rib fracture, sternal fracture, pneumothorax, hemothorax, and pulmonary contusion. BCI should be highly suspected when these other injuries are presents, and these other injuries may greatly affect the patients overall prognosis.
Diagnosis and evaluation
A high index of suspicion as well as careful evaluation of mechanism is essential to the early diagnosis of blunt cardiac injury. The majority of patients are asymptomatic. Those that do complain most commonly complain of chest pain, but this can be confounded by the presence of chest wall injuries. More substantial BCI may manifest as shock, which must be distinguished from other causes of hypotension such as tension pneumothorax, neurogenic and hypovolemic shock.
Numerous modalities have been employed to establish the diagnosis of BCI, including CXR, EKG, Holter monitoring, cardiac enzymes, transthoracic (TTE) and transeesophageal (TEE) echocardiography and nuclear medicine scans. Chest X rays are routinely obtained in trauma patients and may detect chest wall injuries such as rib fractures, which are commonly seen in conjunction with BCI. EKGs are a valuable screening tool and may detect rhythm and conduction disturbances. However, there is no pathonogmotic finding to reliably diagnose BCI. Cardiac enzymes, particularly troponin T, may be elevated in the setting of BCI and measurement of their levels in conjunction with EKG evaluation may aid in diagnosis. Echocardiography can detect segmental wall abnormalities or valvular dysfunction, and generally the tranesophageal route is more sensitive than transthoracic. Hostorically, radionucleotide scans have been used for diagnosis of BCI, but none have been sufficiently sensitive or specific to reliably diagnose BCI. Therefore, their use has since been abandoned.
Spectrum of injury
As mentioned above, the spectrum blunt cardiac injury varies greatly. The AAST organ injury scale is one way of quantifying the extent of injury.
AAST Injury Scale: Cardiac Injuries
Grade I
Blunt cardiac injury with minor EKG abnormality (non specific ST of T wave changes, premature atrial or ventricular contractions, or persistent sinus tachycardia
Blunt or penetrating pericardial wound without cardiac injury, tamponade, or cardiac herniation
Grade II
Blunt cardiac injury with heart block or ischemic changes without cardiac failure
Penetrating tangential cardiac wound, up to but not extending through endocardium, without tamponade
Grade III
Blunt cardiac injury with sustained or multifocal ventricular contracations
Blunt or penetrating cardiac injury with septal rupture, pulmonary or tricuspid incompetence, papillary muscle dysfunction, or distal coronary artery occlusion without cardiac failure
Blunt pericardial laceration with cardiac herniation
Blunt cardiac injury with cardiac failure
Penetrating tangential myocardial wound, up to but not through endocardium, with tamponade
Grade IV
Blunt or penetrating cardiac injury with septal rupture, pulmonary or tricuspid incompetence, papillary muscle dysfunction, or distal coronary artery occlusion producing cardiac failure
Blunt or penetrating cardiac injury with aortic or mitral incompetence
Blunt or penetrating cardiac injury of the right ventricle, right or left atrium
Grade V
Blunt or penetrating cardiac injury with proximal coronary artery occlusion
Blunt or penetrating left ventricular perforation
Stellate injuries, less that 50% tissue loss of the right ventricle, right or left atrium
Grade IV
Blunt avulsion of the heart
Penetrating wound producing more than 50% tissue loss of a chamber
More comprehensively, BCI can be broken down into different injury patterns.
I. Pericardial injury
Pericardial injury results from direct high energy impact or acute increase in intraabdominal pressure. The pericardium ruptures either on the diaphragmatic or pleural surface usually parallel to the phrenic nerve. This may lead to cardiac evisceration and torsion of the great vessels. Clinical presentation may vary from hemodynamic instability to cardiac arrest. In these patients, SCR may reveal displacement of the cardiac silhouette, pneumopericardium, or abnormal gas pattern due to herniated hollow viscera. FAST and EKG may aid in diagnosis. Treatment requires surgical intervention best approached with median sternotomy.
II. Valvular injuries
Valvular injuries are rare in blunt cardiac injury but may have significant sequelae. The most frequently injured valves are the aortic, followed by the mitral. Important clinical findings include the presence of a new cardiac murmur, thrill, or loud musical murmur. Left ventricular dysfunction with cardiogenic shock and pulmonary edema are more significant and ominous symptoms.
III. Coronary artery inuries
Injury to the coronary arteries is extremely rare. Direct impact may cause arterial thrombosis, resulting in intimal disruption and the possibility of MI or ventricular aneurysm potentiating chamber rupture, ventricular failure, and production of emboli or malignant arrhymthmias.
IV. Cardiac chamber rupture
Although uncommon, it is often fatal. Patients that do survive to hospital presentation present with signs of profound hypotension or pericardial tamponade. The right sided chambers are more frequently involved, though left sided injuries as well as multiple chamber injuries have also been reported.
V. Myocardial contusion
Perhaps this is the most common, albeit usually the most innocuous form of BCI. This involves direct injury to the muscle of the heart, generally manifested as EKG changes or elevation in cardiac enzymes. After multiple clinical studies, The Eastern Association for the Surgery of Trauma (EAST) has generated the following guidelines for evaluation and treatment of myocardial contusion.
Level I
Admission EKG should be obtained in all patients where there is suspected BCI
Level II
If admission EKG is abnormal, the patient should be admitted for continuous EKG monitoring for 24-48 hours . If admission EKG is normal, further pursuit of diagnosis should be abandoned.
If the patient is hemodynamically unstable, an imaging study such as TTE or TEE should be obtained.
Nuclear medicine scans add little compared with echocardiography and are not useful if echocardiography has been performed.
Level III
Elderly patients with known cardiac disease, unstable patients, and those with abnormal admission EKGs can be safely operated on provided that they are closely monitored.
The presence of a sterna fracture does not predict the presence of BCI, and does not necessarily indicate that monitoring should be performed.
Neither CPK analysis nor measurement of circulating cardiac troponin T are useful in predicting which patients have or will have complication related to BCI.
Conclusions
Blunt cardiac injuries are generally seen in the setting of high impact trauma. Presentation varies greatly, however more severe injuries may lead to exsanguinations, pericardial tamponade, or death. Therefore, a high index of suspicion, as well as knowledge or the appropriate evaluation and diagnostic work-up, is essential to the optimal care of patients sustaining BCI.
The followings are links to other resources for more information regarding the blunt cardiac injury:
Mattox KL, Flint LM, Carrico CJ et al. Blunt Cardiac Injury. J Trauma 1992; 33:649-650
Roy-Shapira A, Levi I, Khoda J. Sternal Fractures: a red flag or a red herring? J Trauma 1994; 37:59-61
Pasquale MD et al. Practice Management Guidelines for Screening of Blunt Cardiac Injury. Eastern Association for the Surgery of Trauma 1998
Asensio J A et al. Trauma to the Heart in Trauma, 6th edition, Feliciano DV, Mattox KL, Moore EE, Macgraw Hill, New York 2008
Julie Ottosen MD, W Alan Guo, MD, PhD, FACS (November 2012)
Dual chamber cardiac rupture following blunt thoracic trauma
A B S T R A C T
Introduction Cardiac rupture following blunt thoracic trauma is rare. When diagnosed, these injuries have a mortality rate approaching 90%. Although there are reports of dual chamber cardiac rupture, there are no documented survivors from this injury. Case Report A fifty-year-old man presents after high speed motor vehicle crash. On arrival, he was hypotensive with massive right hemothorax. He progressed to asystole but pulse was regained and he went to the operating room. Upon right thoracotomy we encountered a right pericardial laceration and his incision was converted to bilateral thoracotomy (clamshell). He was found to have both right and left atrial rupture. Both injuries were rapidly repaired. The patient survived to discharge neurologically intact. Discussion Cardiac chamber rupture is rare and often fatal. Survival can occur with dual chamber rupture if swift action is taken and all members of the team work together.
Blunt cardiac rupture (BCR) is a rare event. Data from the National Trauma Data Bank (NTDB) reveals that of all blunt trauma patients presenting to the emergency department, only 0.045% sustained BCR [1]. While incidence of BCR in patients arriving to the hospital alive is low, in an autopsy study of 160 fatal cardiac wounds, Fedakar found that only 5% of patients suffering from BCR were admitted to a hospital [2]. This suggests that the vast majority of BCR patients die in the field prior to medical care. Of patients that arrive to the hospital alive, overall mortality of BCR is 89% [1]. Blunt cardiac rupture is not evenly distributed between chambers. In a 5-year review of blunt cardiac rupture Brathwaite and colleagues found right atrial rupture in 41%, right ventricular rupture in 31%, left atrial rupture in 25% and left ventricular rupture in 13% [3]. None of the patients with ventricular or dual chamber rupture survived.
Diagnosing BCR quickly can be challenging. Although the Focused Assessment with Sonography for Trauma (FAST) exam is a useful tool for the diagnosis of BCR when it presents with cardiac tamponade, the diagnosis is often masked when combined with pericardial laceration [4, 5]. While there have been many case reports, retrospective case series, and NTDB studies of BCR, to our knowledge there are no published cases of survival following a dual chamber cardiac rupture from blunt thoracic injury. This unique case was challenging in its presentation and management.
CASE REPORT
A 50-year-old man presented to our Level 1 trauma center following a high-speed motor vehicle collision. There was major damage to his vehicle and his steering wheel had been sheared off the column. At the scene, he had a Glasgow Coma Scale (GCS) 3, shallow breathing and weak pulse. He had decreased breath sounds bilaterally with declining pulse and emergency medical personnel performed bilateral needle decompression. On arrival to the hospital he was apneic with GCS of 3 and faint pulse. He was intubated and bilateral chest tubes were placed. In this process his pulse was lost and cardiopulmonary resuscitation (CPR) was started. His FAST exam was negative and of note, he did not have evidence of tamponade and cardiac ultrasound did not reveal pericardial effusion. He had 1,000 mL of blood from his right chest tube and 300 mL from his left chest tube. Massive transfusion of packed red blood cells, plasma and platelets was rapidly started. After three rounds of CPR, he regained a pulse. Because he continued to have large volume of blood from his right chest tube after his pulse was regained, he was taken directly to the operating room.
In the operating room a right thoracotomy was performed. Given his mechanism and critical state, coupled with the presence of two board certified surgeons, a laparotomy was performed concomitantly. He was found to have a Grade II liver laceration and his abdomen was rapidly packed. His right thoracotomy revealed a massive hemothorax and a pericardial laceration. While his pericardium was being opened, the thoracotomy was extended to the left side with transverse sternotomy (clamshell) for optimal exposure. Upon opening the pericardium, a right atrial appendage rupture was encountered. It was clamped and repaired. He lost his pulse again and received intra-cardiac epinephrine with initiation of manual cardiac message. He regained a pulse and moments later a large volume of bright red blood began to appear from the retro-cardiac space. The posterior portion of the heart was evaluated, and a left atrial rupture was encountered. In a similar fashion, it was clamped and repaired. Hemostasis was achieved, his chest was closed, his abdomen was temporarily closed, and he was returned to the recovery room.
Throughout the surgery the anesthesia team continued with massive transfusion using rotational thromboelastometry (ROTEM) directed correction of coagulopathy. His estimated blood loss was 8 L. He received 30 units packed red blood cells, 30 units fresh frozen plasma, 3 packs of platelets, 6 units of cryoprecipitate and 1,250 mL of autologous blood Post operatively his course was complicated by atrial fibrillation that was reversed medically and controlled with medication. The patient made a full neurologic and physical recovery and was discharged home.
DISCUSSION
Cases or blunt cardiac rupture are rare with exceptionally high mortality rate. There are no documented cases of survival with dual chamber rupture. There are two key components to survival. First, the patient must be rapidly assessed and transported to definitive care. In this case, time of arrival to incision in the operating room was 32 minutes, including CPR, chest tubes, intubation, resuscitation and transport. Secondly, aggressive balanced resuscitation facilitated the surgical team completing the operating, avoid coagulopathy and maintain perfusion to vital organs
Case reports of atrial and pericardial rupture from blunt cardiac trauma
Blunt cardiac trauma is diagnosed in less than 10% of trauma patients and covers the range of severity from clinically insignificant myocardial contusions to lethal multi-chamber cardiac rupture. The most common mechanisms of injury include: motor vehicle collisions (MVC), pedestrians struck by motor vehicles and falls from significant heights. A severe complication from blunt cardiac trauma is cardiac chamber rupture with pericardial tear. It is an exceedingly rare diagnosis. A retrospective review identified only 0.002% of all trauma patients presented with this condition. Most patients with atrial rupture do not survive transport to the hospital and upon arrival diagnosis remains difficult.
Case presentation
We present two cases of atrial and pericardial rupture. The first case is a 33-year-old female involved in a MVC, who presented unresponsive, hypotensive and tachycardic. A left sided hemothorax was diagnosed and a chest tube placed with 1200 mL of bloody output. The patient was taken to the OR emergently. Intraoperatively, a laceration in the right pericardium and a 3 cm defect in the anterior, right atrium were identified. Despite measures to control hemorrhage and resuscitate the patient, the patient did not survive.
The second case is a 58-year-old male involved in a high-speed MVC. Similar to the first case, the patient presented unresponsive, hypotensive and tachycardic with a left sided hemothorax. A chest tube was placed with 900 mL of bloody output. Based on the output and ongoing resuscitation requirements, the patient was taken to the OR. Intraoperatively, a 15 cm anterior pericardial laceration was identified. Through the defect, there was brisk bleeding from a 1 cm laceration on the left atrial appendage. The injury was debrided and repaired using a running 3–0 polypropylene suture over a Satinsky clamp. The patient eventually recovered and was discharged home.
Conclusions
We present two cases of uncontained atrial and pericardial rupture from blunt cardiac trauma. Contained ruptures with an intact pericardium present as a cardiac tamponade while uncontained ruptures present with hemomediastinum or hemothorax. A high degree of suspicion is required to rapidly diagnose and perform the cardiorrhaphy to offer the best chance at survival.
Blunt cardiac trauma is diagnosed in less than 10% of trauma patients and covers the range of severity from clinically insignificant myocardial contusions to lethal multi-chamber cardiac rupture [1]. The most common mechanisms of injury include: motor vehicle collisions (MVC) (50%), pedestrians struck by motor vehicles (35%), motorcycle crashes (9%), and falls from significant heights [2]. In one autopsy study, cardiac injury was identified in 11.9% of over 1600 fatalities from blunt trauma and was either the only cause of death or contributed to the fatal outcome in 45 to 76% of those cases [2, 3, 4]. Although blunt traumatic atrial tears have been reported to have a better prognosis than ventricular ruptures, these injuries remain rapidly fatal and require a high index of suspicion and emergent operative repair [4, 5, 6].
Blunt traumatic rupture of the heart and pericardium, rarely diagnosed preoperatively, carries a high mortality rate. The National Trauma Data Bank reports that chamber rupture represents 0.041% of all trauma cases and has an overall mortality rate of 89.2% [7]. A retrospective review of more than 20,000 patients admitted from 1979 to 1989 to a single Level I trauma center identified 59 (0.002%) patients requiring emergency surgery for this condition. The overall mortality rate was 76% (45 patients), and only 52% for those with vital signs on admission [8]. A similar study showed 11 patients out of 58,304 (0.0002%) trauma activations were diagnosed with blunt cardiac rupture over a five year period [9]. Finally, in a review of 4169 victims of traffic collisions fatally injured between 1972 to 1985, chest injuries were recorded as the main cause of death in 1121 victims. Despite wearing a seatbelt, 75 out of 207 patients were found to have cardiac rupture on autopsy. In frontal impact collisions, the mechanism leading to cardiac rupture is usually a crushing force against the steering wheel, with increasing severity depending on vehicle mass and velocity [10].
Most patients with atrial rupture do not survive transport to the hospital. In those who present to hospitals, diagnosis remains difficult. Traditionally, blunt cardiac rupture with an intact pericardium presents with signs and symptoms of cardiac tamponade. Whereas, cardiac rupture with torn pericardium present with hemomediastinum or hemothorax [11]. When evaluating a hemothorax from blunt trauma, atrial rupture with combined pericardial rupture remains low on the differential but cannot be neglected. We present two cases to illustrate this rare diagnosis.
We present the case of a 33-year-old female who was an unrestrained driver in a MVC with major front-end damage where airbags were deployed. She arrived to Advocate Christ Medical Center (a high volume, academic, level 1 trauma center) unresponsive with a Glasgow Coma Scale (GCS) of 5 and was intubated for airway protection. Breath sounds were noted to be present bilaterally. She was tachycardic and hypotensive with a heart rate of 143 and blood pressure of 71/46. A focused assessment with sonography for trauma (FAST) demonstrated no evidence of intra-abdominal or pericardial fluid. A left sided hemothorax was present on chest x-ray, and a chest tube was placed with 1200 mL of bloody output initially (See Fig. 1). At this point, the decision was made to take patient emergently to the operating room (OR) for exploration.
Fig. 1
Case 1: Left sided hemothorax
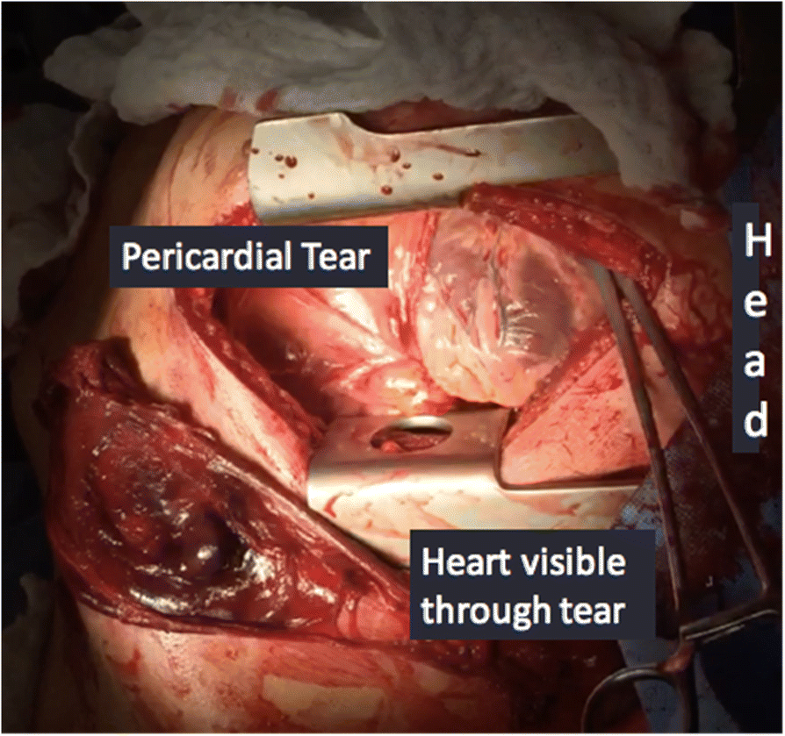
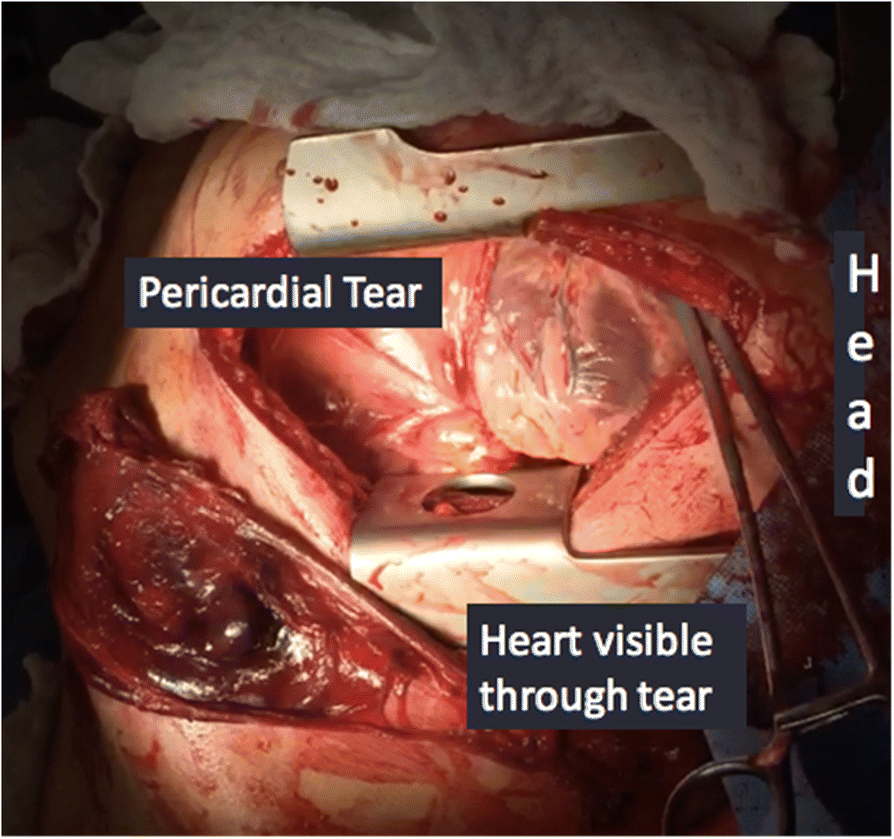
A left anterolateral thoracotomy incision was made with the patient in a supine position. There was a significant amount of blood upon entry into the chest cavity, and there was no cardiac tamponade. Despite cross clamping the pulmonary hilum, the bleeding continued. While being resuscitated with the massive transfusion protocol, there was no end tidal CO2 noted. The pericardium was opened, heart delivered, and cardiac massage was started. A separate defect in the superior, right side of the pericardium was found as well as a 3 cm defect in the anterior right atrium (See Fig. 2). Despite measures to control hemorrhage and resuscitate the patient, the patient did not survive. The blood loss was greater than 6 l.
The second case is a 58-year-old male who was involved in a high-speed MVC. The patient had a prolonged extrication from his vehicle and was intubated after being found unresponsive. On arrival his GCS was 3 T. He was hypotensive with FAST negative for intra-abdominal blood, but a large left hemothorax was identified on the left upper quadrant view. A chest tube was placed with initially 900 mL of blood out followed by 200 mL per hour for 2 h. Based on the output and ongoing resuscitation requirements, the decision was made to take the patient to the OR.
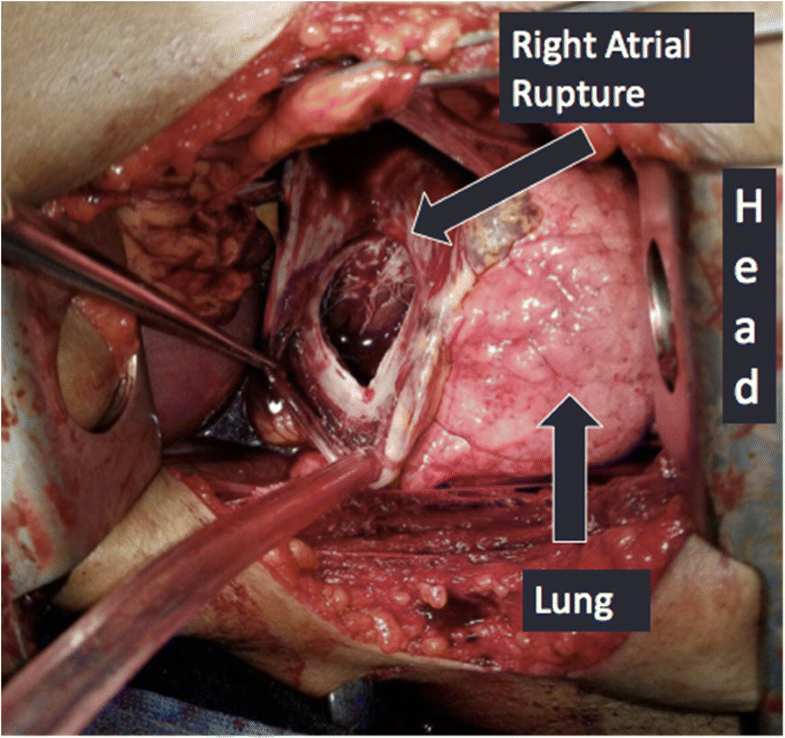
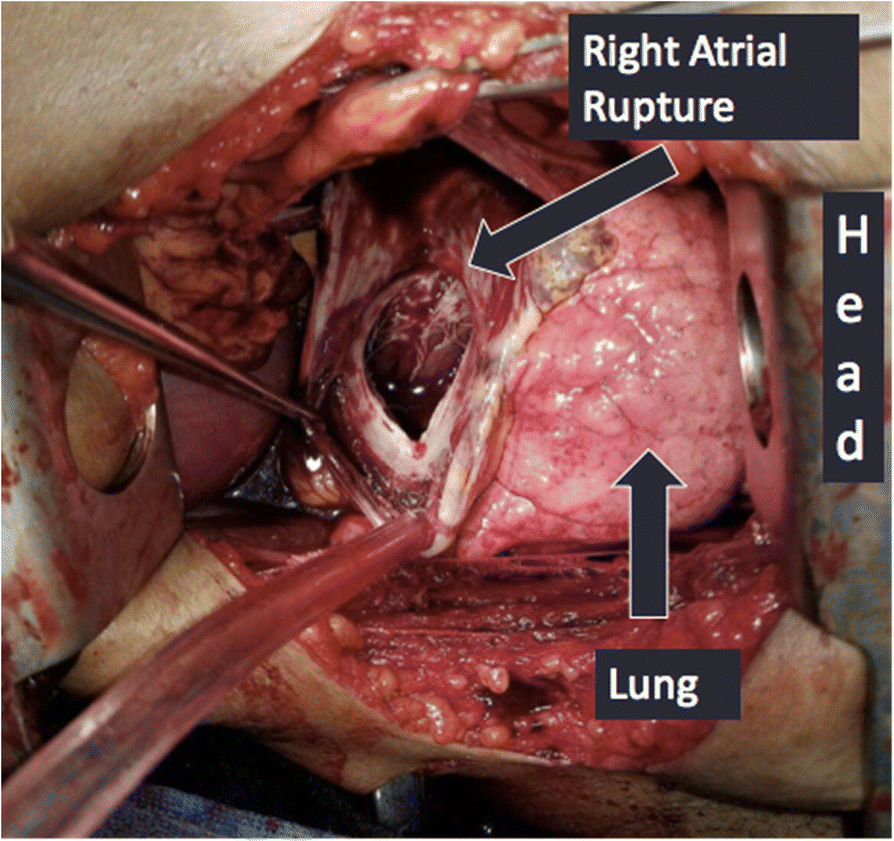
A left anterolateral thoracotomy incision was made with the patient in supine position. There was approximately 1 L of clotted blood within the chest cavity coming from an anterior pericardial laceration, about 15 cm in length. Through the defect there was brisk bleeding coming from a 1 cm laceration on the left atrial appendage (See Fig. 3). The injury was debrided and repaired using a running 3–0 polypropylene suture over a Satinsky clamp. The pericardial defect was closed to prevent cardiac herniation. The patient recovered well and was eventually discharged home.
Fig. 3
Case 2: Pericardial tear with left atrial appendage laceration
In our case series, we present two patients who were taken to the OR with uncontained blunt cardiac rupture. With a 89.2% mortality rate for chamber rupture [7], most of these patients do not make it to the hospital, let alone the OR. With such a high mortality rate, we feel it is important to review these cases to discuss their presentations and treatment options.
The first patient arrived unresponsive, tachycardic and hypotensive after blunt trauma. Following Advanced Trauma Life Support (ATLS) principles, the patient was intubated and resuscitation started. The FAST exam was performed, and failed to show any pericardial effusion. This was due to the rupture not only of the right atrium, but the pericardium itself. This allowed exsanguination into the pleural space. From autopsy data, fatal blunt cardiac trauma with chamber rupture occurs most often to the left ventricle [6, 10]. In contrast, in patients that present to the hospital, right atrial rupture is more common. These injuries are seen at the superior vena cava-atrial junction, inferior vena cava-atrial junction or in right atrial appendage (a common site of rupture due to its thin wall) [6, 10].
Pericardial tears often occur secondary to increased intra-abdominal pressure or lateral decelerative forces from either side. In blunt injury with cardiac rupture, 70% of the time the pericardium stays intact; in 30% of cases it ruptures [12]. Cardiac herniation with cardiac dysfunction can occur in conjunction with these tears. The heart may be displaced into either the pleural cavity or even into the abdomen depending on the location of the pericardial defect. In right-sided pericardial rupture, the heart can twist along the caval axis, preventing venous return, and leading to the surprising discovery of an empty pericardial cavity during a resuscitative left anterolateral thoracotomy [1].
Alternatively, patients may bleed into the mediastinum or into the pleural cavity. This often leads to a delay in diagnosis. This is not surprising, as most pericardial ruptures will be diagnosed with thoracotomies in the OR [8]. May et al. (1999) describes two similar cases in which the patients had cardiac and pericardial ruptures. Ultimately, the patients succumbed to their injuries due to exsanguination into the mediastinum and thorax [11]. This unfortunately, was the same result as our first case.
The second patient presented with left sided hemothorax after a MVC. The differential of left sided hemothorax after blunt injury is broad and ranges from intercostal artery injury or lung parenchyma laceration to great vessel or cardiac injury. Cardiac rupture is a rare etiology of hemothorax. In a recent series of cases, Oizumi et al. [12] describes only 11 known patients who have survived blunt cardiac rupture with a concomitant pericardial defect [12]. Our patient would perhaps be the 12th.
Desforges and coauthors reported the first repair of a blunt myocardial rupture in 1955, successfully closing a right atrial perforation secondary to a MVC [13]. The traditional approach for a left-sided hemothorax is a left anterolateral thoracotomy. To improve access to the heart, the incision can be extended with to a median sternotomy or a right anterolateral thoracotomy incision. In situations where primarily a cardiac injury is suspected, it would be appropriate to start with a median sternotomy. A left thoracotomy often does not provide adequate exposure to the heart or ascending aorta.
For cardiac lacerations, cardiorrhaphy can be accomplished via several techniques. Methods to temporize bleeding to allow time for definitive repair include the use of a foley balloon through the defect to occlude the opening or temporary closure with direct pressure, staplers or vascular clamps [1]. Definitive repair with double armed monofilament pledgeted suture repair either an interrupted or running technique has been described [9, 14]. If large septal defects, uncontrollable bleeding or coronary artery injury is identified intraoperatively, consultation with a cardiothoracic surgeon is recommended. The patient may need cardiopulmonary bypass or extracorporeal life support to allow for definitive repair. If the patient is able to survive the initial insult, heart failure may ensue requiring assist devices or even transplant [9].
In summary, we present two cases of uncontained atrial rupture from blunt cardiac trauma. Contained ruptures with an intact pericardium can present as a cardiac tamponade while uncontained ruptures present with hemomediastinum or hemothorax and are more likely to be fatal. A high degree of suspicion is required to rapidly diagnose and perform the cardiorrhaphy to offer the best chance at survival.
Department of Surgery, Division of Surgical Critical Care, University of Illinois at Chicago.
Department of Trauma, Division of Trauma /Surgical Critical Care, Advocate Christ Medical Center.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
DB and JL were present in the operation of case one. EO was present in the operation of the second case. DB was the primary author of the case reports. KC and HM contributed in writing the discussion and conclusion sections. All authors read and approved of the final manuscript.
Authors’ information
DB, KC, HM are general surgery residents at the University of Illinois-Chicago.
JL and EO are attending trauma surgeons at Advocate Christ Medical Center.
Ethics approval and consent to participate
Not applicable.
Consent for publication
All participants have agreed and consented to be included in this case report. The images, figures or patient data used are included in this consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Fulda G, Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley RA. Blunt traumatic rupture of the heart and pericardium: a ten-year experience (1979-1989). J Trauma. 1991;31(2):163–7.View ArticleGoogle Scholar
Leavitt BJ, Meyer JA, Morton JR, Clark DE, Herbert WE, Hiebert CA. Survival following nonpenetrating traumatic rupture of cardiac chambers. Ann Thorac Surg. 1987;44(5):532–5.View ArticlePubMedGoogle Scholar
Fulda G, Brathwaite CE, Rodriguez A, et al. Blunt traumatic rupture of the heart and pericardium: a ten-year experience (1979 to 1989). J Trauma. 1991;31:167–73.View ArticlePubMedGoogle Scholar
Nan YY, et al. Blunt traumatic cardiac rupture: therapeutic options and outcomes. Injury. 2009;40(9):938–45.View ArticlePubMedGoogle Scholar
Santavirta S, Arajarvi E. Ruptures of the heart in seat belt wearers. J Trauma. 1992;32(3):275–9.View ArticlePubMedGoogle Scholar
May AK, Patterson MA, Rue LW 3rd, Schiller HJ, Rotondo MF, Schwab CW. Combined blunt cardiac and pericardial rupture: review of the literature and report of a new diagnostic algorithm. Am Surg. 1999;65(6):568–74.PubMedGoogle Scholar
Desforges G, Ridder WP, Lenoci RJ. Successful suture of ruptured myocardium after nonpenetrating injury. N Engl J Med. 1955;252:567–9.View ArticlePubMedGoogle Scholar
Telich-Tarriba JE, et al. Surgical repair of right atrial wall rupture after blunt chest trauma. Tex Heart Inst J. 2012;39(4):579–81.PubMedPubMed CentralGoogle Scholar






Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου