Case
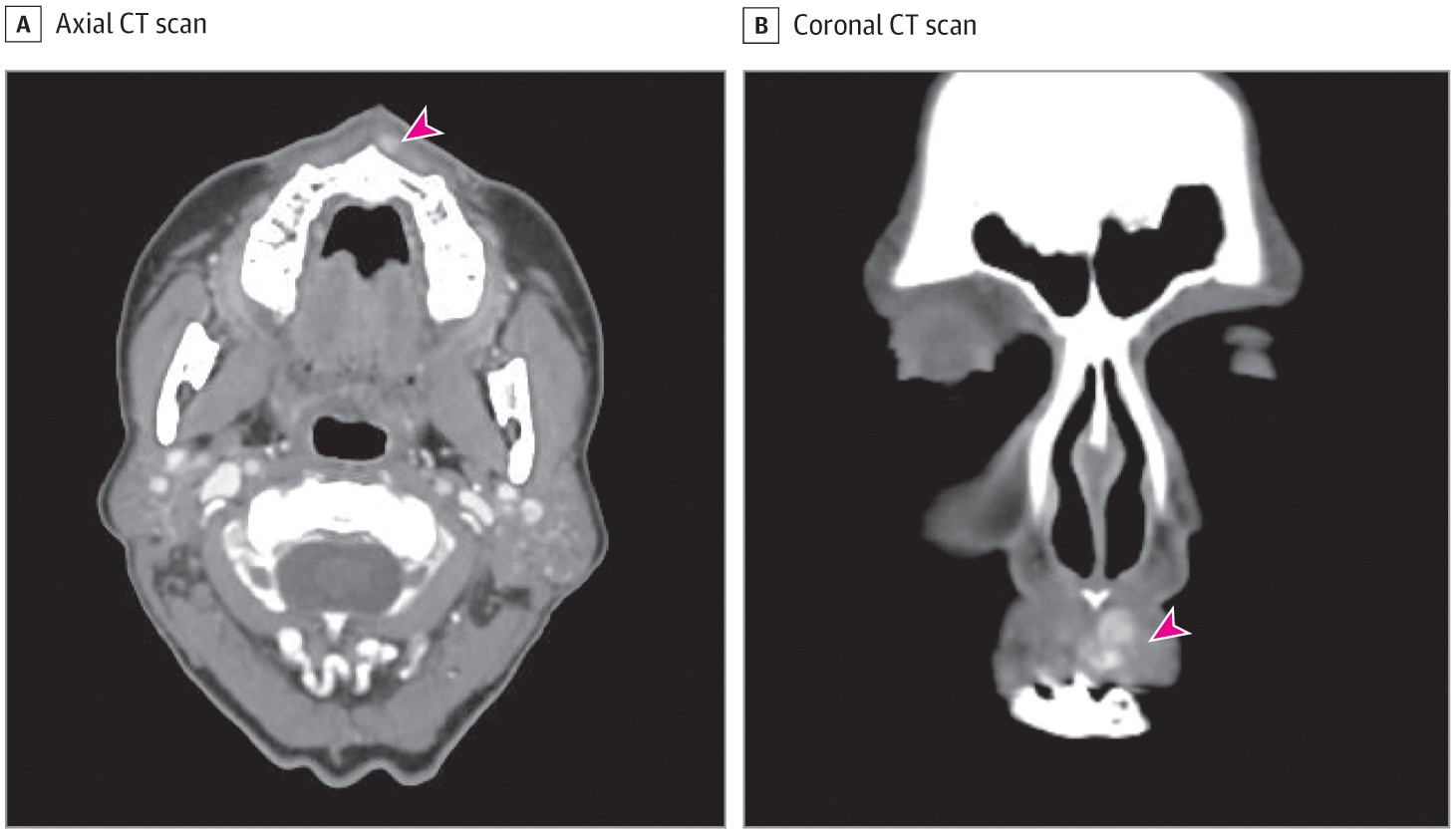
Awoman in her 60s reported right upper lip submucosal masses that had been present for several weeks. She denied associated pain, bleeding, or recent trauma to the lip. She also denied any other constitutional symptoms. Her social history was significant for a 45–pack-year smoking history and social drinking. On physical examination, the patient had right upper lip submucosal masses without any tenderness or mucosal abnormality. The remainder of the otolaryngic examination was unremarkable. A computed tomographic scan of the neck with contrast demonstrated multiple hyperenhancing nodules; the largest was 3 × 7 × 6 mm, with no local bony erosion or cervical lymphadenopathy (Figure 1).
{kind=link}
What Is Your Diagnosis?
- Multifocal basal cell adenoma
- Basal cell adenocarcinoma
- Multifocal canalicular adenoma
- Adenoid cystic carcinoma
Discussion
Diagnosis
C. Multifocal canalicular adenoma
Canalicular adenoma is an uncommon salivary gland tumor arising almost exclusively from the minor salivary glands of the oral cavity. It is usually asymptomatic and slow growing, and accounts for less than 1% to 3% of all salivary neoplasms.1,2 Canalicular adenoma is most commonly diagnosed as an upper lip nodule found in women in their seventh decade of life, as exemplified by our patient.1 Other locations in which canalicular adenoma can be found include the hard palate and buccal mucosa.1 It is the third most common benign salivary gland tumor, with a recurrence rate of approximately 5%.1,2 Canalicular adenoma was previously thought to be a variant of basal cell adenoma; however, its unique clinical and pathologic features warrant defining it as its own entity.3 For example, while canalicular adenoma is seen almost exclusively in the oral cavity, basal cell adenoma has a predilection for the major salivary glands, especially the parotid gland.2-4 This locational difference is the first hint in differentiating between these 2 entities.
Histologically, canalicular adenoma tends to be a well-circumscribed solitary nodule consisting of anastomosing cords formed by columnar cells arranged in a loose connective tissue stroma.1,2 As seen in this patient, however, approximately 15% of canalicular adenomas are multifocal, a feature that must not be misinterpreted as invasive growth, a defining feature of salivary gland carcinomas such as adenoid cystic carcinoma or basal cell adenocarcinoma. By immunohistochemistry, canalicular adenoma is consistently positive for S100 and SOX10, variably positive for p63, and negative for p40.1,2 Although basal cell adenoma is also composed of basaloid cells growing as nests and cords, it exhibits a more cellular stroma and has 2 cell populations: basaloid myoepithelial cells and ductal cells; the myoepithelial cells can by highlighted by immunohistochemistry for smooth muscle actin, calponin, glial fibrillary acidic protein, and others.5 More important, canalicular adenoma is composed of 1 population of ductal cells, and does not stain for myoepithelial elements that are found in basal cell adenoma, basal cell adenocarcinoma, and adenoid cystic carcinoma.4 Surgical resection is the treatment of choice for canalicular adenoma.1 In contrast, malignant neoplasms such as adenoid cystic carcinoma may need further management with radiotherapy and frequent monitoring, making differentiation imperative.6
Clinically, canalicular adenoma may mimic a mucocele, which is a collection of mucus in the soft tissue after rupture of a salivary gland duct.4,7 Both can present as well-demarcated blue-tinted masses or even match the color of normal oral mucosa.7 Unlike canalicular adenoma, mucoceles are often associated with a history of trauma, which our patient denied.7 In addition, mucoceles are often diagnosed earlier in life, around the second decade, and are found equally in males and females.7 Mucoceles are found predominately in the lower labial mucosa with virtually no presentation in the upper labial mucosa, making this diagnosis unlikely for our patient.7 Histologically, the differentiation is simple, with mucocele histologic characteristic showing mucin in a subepithelial vesicle.7
In summary, histologic characteristics and immunohistochemistry are crucial for distinguishing canalicular adenoma from other diagnoses. Canalicular adenoma is occasionally multifocal, a feature that must be distinguished from the truly invasive growth that characterizes similar-appearing malignant neoplasms. Although surgical resection is the mainstay of treatment for upper lip masses, differentiation is necessary in cases in which the diagnosis of adenoid cystic carcinoma necessitates concurrent use of radiotherapy. Other factors such as patient sex, decade of life, and location of mass are also helpful in the initial formation of a differential diagnosis.
Patient Outcome
After surgical excision, pathologic examination revealed a nodular proliferation of basaloid cells (Figure 2A) made up of nodules ranging from less than 1 to 7 mm. In the background minor salivary tissue, there were several additional microscopic, incipient nodules with an identical appearance (Figure 2B). The nodules were composed of nests and interconnecting cords of uniform cells with bland, elongated nuclei with vesicular chromatin and delicate nucleoli. The tumor cells were set in a loose myxoid stroma (Figure 2C). Although the tumor was multinodular, no convincing invasive growth was seen. By immunohistochemistry the tumor was diffusely positive for S100 and SOX10, focally positive for p63, and negative for p40.
Figure 2.
{kind=link}

Staining of excised mass reveals nodular proliferation of basaloid cells (hematoxylin-eosin, original magnification x40) (A); microscopic, incipient nodules (black arrowheads) in the background minor salivary gland tissue (hematoxylin-eosin, original magnification x100) (B); and tumor cells in loose myxoid stroma (hematoxylin-eosin, original magnification x200) (C).
Back to top
Article Information
Published Online: February 28, 2019. doi:10.1001/jamaoto.2018.4363
Conflict of Interest Disclosures: None reported.
Additional Contributions: We thank the patient for granting permission to publish this information.
References
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου